
Mental Illness Stigma in Turkish and Greek Cypriot Communities Living in Cyprus: A Pilot Study

Abstract
Currently stigma is considered to be the most important factor in the field of mental illness. More than 40 types of negative impact of stigma on ones’ life has been identified for the previous researchers. Although the impact of it is very negative there has not been any study conducted in the Northern side of Cyprus where Turkish Cypriots live. There has also very limited studies carried out in the Southern side where Greek Cypriots live. The aim of this study was, therefore, to investigate the attitudes of the Greek and Turkish Cypriot populations living in Cyprus towards schizophrenia and look into the possible explanations behind these differences. An independent groups design was used in this study. One hundred participants were recruited from Greek and Turkish Cypriot populations. Participation to this study was voluntary and participants were represented with four different questionnaires assessing knowledge regarding mental health, attitudes towards mentally ill, level of familiarity and culture. The results showed that there was a significant difference between the Turkish and Greek Cypriot attitudes towards schizophrenia; Turkish Cypriots held more negative attitudes. Turkish Cypriots were also significantly more vertical collectivist, which was associated with the higher levels of stigma. Furthermore, Greek Cypriots were significantly more familiar with mental health problems and were found to have higher levels of knowledge about schizophrenia.
Keywords: Public Stigma, horizontal-vertical ındividualism-collectivism, cyprus, prejudice, discrimination
Introduction
Public stigma has been defined by Corrigan, Rowan, Green, Lundin, River, Uphoff-Wasowski, White, and Kubiac, (2003) as a status loss and discrimination of individuals with mental health problems due to negative prejudice from the general public. Norman, Sorrentino, Gawronski, Szeto, Ye and Windell (2010) further explained stigma as a complex process that is cognitive and behavioural which takes place between the general public and mentally ill individuals. Stereotypes refer to the beliefs that are negative and associated with mentally ill individuals such as dangerousness and unpredictability (public stigma) and incompetency (self-stigma) (Pingani, Forghieri, Ferrari, Ben-Zeev, Artoni, Mazzi, and Corrigan, 2011). Prejudice, such as fear (public stigma) and low self-esteem (self-stigma) are cognitive and emotional responses that are activated by the stereotypes. These may then lead to discrimination, which is a behavioural response to prejudice; not employing someone due to his or her mental health problem (public stigma) or not applying for a job due to having a mental illness (self stigma).
Two main theoretical models on stigma have been developed in an effort to explain how it forms; labelling (Link et al., 1987) and attribution theories (Corrigan, 2000). Scheff’s original theory of labelling suggested that stereotypes about mental illness are learnt at an early age through social interactions and media, which are then internalized and applied to self in the case of mental illness. Individuals diagnosed with mental illness are aware of these roles that expected from them by the public, they therefore, start acting in such way. According to this theory, once someone is diagnosed with mental illness a new identity of a “psychiatric patient” and a social status is created for that individual. Stigma is then formed which is expressed as labelled individual being excluded form the daily interactions (Link et al., 1987). Another theory that sought to understand the stigma of mental illness is attribution theory (Heider, 1958). Corrigan (2000) developed Weiner’s original attribution theory and applied it specifically to stigma of mental illness. According to him, there are 3 constructs of mental illness stigma; signalling event, cognitive and affective responses and behavioural reaction. There are signals such as poor social skills, which may indicate that there may be something unusual or alarming about the individual. Similar to Weiner, Corrigan also suggested that if the illness is attributed to an external factor the person is more likely to receive pity, therefore, help and less negative attitudes. This is opposite for those who are held responsible for their illness which in turn receive more anger and punishing behaviour consequently more stigma.
Furthermore, a widely used social-psychology model has further been developed which adopted aspects from both attribution and labelling theories (Angermeyer & Matschinger, 2003, Angermeyer, Matschinger, & Corrigan, 2003; Corrigan, Edwards, Green, A., Diwan, & Penn, 2001). Corrigan et al., (2000) suggested that this model claims that stigmatizing attitudes are constructed due to ones previous experience and knowledge which then leads to a behavioural response. A casual pathway model consists of experience, perception, affect and response (See Figure 1).
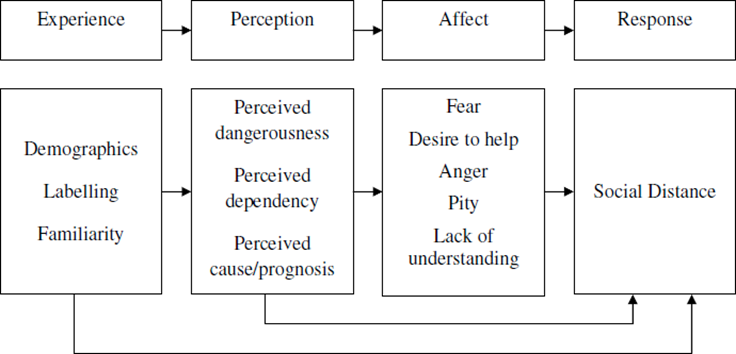
In detail, this model considers perceptions and affects as attribution, which in turn results in discrimination as a behavioural response (Emmerton, 2010). Unlike the labelling and the attribution theories this model also considers other factors, which are identified as contributors to the stigma of mental illness; demographics and familiarity.
According to the researchers stigma commonly results in economical, personal, political and social challenges for those who have such health conditions (Halter, 2008). Attitudes that are stigmatizing may also result in discriminative behaviour; restriction of someone’s everyday life practices as well as prospects in public and private institutions. Many researchers also suggested that stigma may prevent individuals from engaging with others in the societies which in turn may worsen their condition (Vauth, Kleim, Writz, & Corrigan, 2007; Mojtabai, 2010). Considering these negative effects understanding the attitudes and beliefs of the general public about mental illness is very important. Ajzen and Fishbein, (1980) noted that this is particularly fundamental when trying to identify the causes behind stigmatizing attitudes, as the beliefs and attitudes have been found to be good predictors of behaviour, consequently enabling stigma reduction.
Particularly knowledge and contact are the most identified factors, which have been found to contribute to stigma levels by the researchers. Previous research suggests that the general public lack understanding of the nature and causes of mental illness; contributing to the negative attitudes and subsequently stigma of mental health problems (Thornicroft, Rose, Kassam and Sartorius, 2007). For example, Jorm, Christensen, and Griffiths (2005) carried out a study assessing the impact of knowledge on stigma in Australia. They compared two groups; one which received a well- organized education on depression and its treatments, while the other group did not. Upon comparing these, they found that the group that received education held more favorable attitudes, were more likely to correctly recognize and identify depression, and support professional treatment.
The second group, alternatively, held less favorable attitudes towards depression and its treatment. In Sorsdahl and Stern’s (2010) study, it was found that most of the South African participants were unable to identify mental illness from the vignette that was represented to them and this was associated with higher negative attitudes. They also noted that the most negative attitudes were shown towards schizophrenia; many viewed these individuals as violent and unpredictable indicating the impact of lack of factual knowledge on stigma.
A study conducted by Unnever and Cullen (2009) argued that stigma levels towards mental illness is reduced if the familiarity is increased because similarity enables greater tolerance and reduces negative attitudes and stigma. Similarly, Corrigan, Green, Lundin, Kibuak, and Penn (2001) conducted a study examining the link between familiarity of mental illness and stigmatizing of someone with a serious mental illness. 208 students were represented with 3 scales; familiarity, dangerousness, fear and social distance. Results of the pathway analysis suggested that those with higher levels of familiarity reported less negative attitudes related to perception of dangerousness and fear, as well as less desire to be socially distant from someone with a serious mental illness.
Although not many studies considered the impact of culture on stigma, according to Won Pat- Borja, Yang, and Phelan (2013) culture and cultural beliefs also play a great role on the stigmatizing attitudes towards individuals with mental health problems. Parkar, Dawani and Apte (2001) noted that defining culture is particularly difficult due to the disagreement amongst the anthropologists regarding the nature of it. For example, in 1952 Kroeber and Kluckhohn conducted a review of the definitions and identified 164 different ones thus making it harder to have a commonly agreed definition. Two of the most commonly used definitions are ‘.’ Tyler (British anthropologist) 1870: 1; cited by Avruch 1998: 6. ‘.’ (Kroeber & Kluckhohn 1952, p. 181; as cited by Adler 1997, p. 14).
Researchers such as Littlewood (1998) and Kirmayer (2001) stated that culture is particularly important in the field of mental illness as cultural variations may influence the way people identify, understand, express and associate with the mental disorders and their treatments subsequently affecting the stigma associated with such conditions. For example, a study showing the impact of culture on mental illness stigma was conducted by Mellor, Carne, Shen, McCabe, and Wang (2013) on participants from Australia and Taiwan. Participants were asked to complete an attitude scale and a scale assessing cultural values. Result from this study showed that immigrant Chinese and Taiwanese group held the most stigmatizing attitudes to mental illness. In addition to this, a significant association between lower stigmatizing attitudes and adaption to Australian culture was found. Australian born Chinese participants showing lower negative attitudes consequently lower stigma levels compared to Chinese immigrants and Taiwanese participants. Furthermore, Hampton and Sharp’s (2014) study showed that compared to Caucasian Americans and Asian Americans Latino Americans held the most stigmatizing attitudes towards mental illness.
Cyprus is a small island in the Eastern Mediterranean at the junction of Africa, Asia and Europe. The ancient Greeks initially colonized the island until the Ottoman Turks took control in 1571. The Ottoman period in the island was significant as it has brought 20% Turkish Cypriots in addition to the native Greek Cypriots to the island; who were the offspring of Turkish origin soldiers and colonizers. With the Lausanne treaty in 1923 the control of the island was given to Britain from Turkey until the independence in 1960. Cyprus conflict has picked up in 1963 after the British colonial period ended there was an increase desire of “ENOSIS” by the Greek Cypriots which meant unification of the island with Greece. On the other hand, Turkish Cypriots were striving for equal status and partition of the island (Papadakis et al., 2002). The conflict and clashes between the 2 major ethnic groups in the island lasted until 1974 and ended by the invasion of the Turkish army. This invasion by Turkey resulted in the division of the island into two parts via “Yesil hat” or “Green Line” where Greek Cypriots immigrated to the Southern side and the Turkish Cypriots immigrated to the Northern side of it. Presently, the island is still divided keeping the ethnic conflict as a hot topic on the island. Cyprus conflict, therefore, consists of several interacting components which are politics, culture, ethnicity and peoples’ identity (Boatswajn, 2005). Sellers, Smith, Shelton, Rowley, and Chavous (1998) argued that ethnic identity of a community includes common name, shared history, cultural norms and values, language and identification with the same homeland. In the case of Cyprus, two different ethnicities; Turkish and Greek were created due to the individuals’ significant identification with what they considered as their motherland; Greece and Turkey. Thus, enabling the two major societies to differ in regards to identity, culture, religion, language, education system and policies and regulations. The doors were opened in 2004 enabling Greek and Turkish Cypriots to interact again after 30 years, which may also allow them to benefit from each other in the case of stigma of mental illness. Before one can do this, the level of stigma and the possible contributor factors should, however, be identified in the both sides.
Several studies have been conducted with Greek and Turkish populations in regards to their attitudes towards mental health problems. For example, Economou et al. (2009) conducted a comparison study with the general public in Greece, Canada (Stuart and Arboleda-Florez, 2001) and Germany (Gaebel et al., 2002) survey results. According to them their results Greek public showed significantly higher willingness to be socially distant from mentally ill individuals compared to Canadian and German public members. This was particularly found when there was a higher intimacy needed in social situations. In addition to this, negative attitudes were mostly found in regards to schizophrenia, which was highly associated with criminality in the Greek societies. It was also found that half of the participants from Greece stated that it would disturb them if they had to work with an individual diagnosed with schizophrenia. This was the case for one out of six German and Canadian public members. A further comparison study was conducted by Papadopoulos et al. (2002) examining the attitudes of White-English and Greek/Greek Cypriots’ living in UK towards mental health problems. In this study, Greek/Greek Cypriot participants were found to be more controlling in regards to mentally ill and they perceived individuals with mental health problems to be less intelligent as opposed to the White English participants. According to Papadopoulos et al. (2002) although Greek/Greek Cypriot participants perceive individuals with mental health problems as less able and mental illness as something to be kept under controlled for safety of the others. A recent study by Panayiotopoulos et al. (2011) compared the Greek Cypriot mental health professionals’ and the general population’s attitudes towards mental health problems. They found that the negative attitudes towards mental illness exist amongst both groups. According to them professionals were, however, significantly more stigmatizing towards mental health problems, they were also less optimistic regarding the ability of such individuals (Panayiotopoulos et al., 2011). This was due to the lack of mental health training given to the professionals such as social workers. Another study came from Poliniki (2011) who compared the attitudes of general health professionals working in primary care and the general population. His results showed that the general public held significantly more negative attitudes towards mental illness compared to the health professionals. There are no studies assessing the attitudes of Turkish Cypriots. Several studies, however, have been conducted in different regions and social settings in Turkey. For example, according to Eker (1989) and Eker and Arkar’s (1994) study amongst the Turkish participants paranoid schizophrenia was the most recognized but the least accepted mental health problem. Arkar and Eker (1994) also found that people are more willing to distance themselves with a person who is diagnosed with paranoid schizophrenia as opposed to someone with a diagnosis of withdrawn schizophrenia or major depression. In addition to this, they also noted that dealing with such individuals would require more emotional and physical effort.
Problem Statement
Although much global research on stigma of mental illness has been carried out (Pinfold, Toulmin, Thornicroft, Huxley, Famer and Graham, 2003), few studies have been done in Cyprus and only including Greek Cypriots. No studies have been carried out on the island comparing the attitudes of the two major ethnicities. This makes it harder to have a clear picture on the attitudes that exist and factors contributing to these. In order to reduce stigma and the negative impact of it on individuals and on societies in general these should be identified.
Research Questions
•Are there any differences between Turkish and Greek Cypriot societies’ attitudes towards mental health problems?
•Where do Turkish and Greek Cypriot societies fit in within the collectivism- individualism cultural dimensions?
•Do knowledge, familiarity and culture affect the level of stigma?
Research Methods
Considering the lack of studies in this field in Cyprus the aim of this study is to assess the attitudes towards schizophrenia and the possible factors influencing these attitudes consequently measuring stigma levels in both Turkish and Greek Cypriot Societies.
Research Methods
Participants
100 people were recruited for this study. 51 of these defined themselves as belonging to the Turkish Cypriot cultural group whereas 49 of the participants defined themselves as belonging to the Greek Cypriot cultural group. The distribution of the age, gender and ethnicity are considered to be balanced across the two participant groups (See Table 1). Greek Cypriots were slightly younger as opposed to Turkish Cypriots with an age mean of 26-35 and 36-50 respectively (Please see Figure 1). Most of the participants were university graduates who worked in public services; including teachers, doctors, nurses, bankers and policy makers (Please see Table 1). Participation to this study was voluntary. They were not known to the researcher and were recruited through mutual contacts.
Materials
Demographic information was obtained from the participants using a demographic questionnaire. They were then represented with two vignettes one which described a man with general life stress (Control Vignette) and the other one that describes a man with schizophrenia. Participants were then asked to rate statements such as ‘I think this person has mental health problem’. Attitudes towards mental illness were then assessed using the Corrigan’s 27-Item Attribution Questionnaire (AQ-27). This scale consists of nine sub-scales which are anger, fear, dangerousness, pity, coercion, responsibility, help, segregation and avoidance (Luty & Varughese, 2010). The participants were given a statement about a person (Harry (GC)/Kemal (TC)) with schizophrenia and were then asked to rate their answers on a Likert scale from 1 to 9 about the questions such as ‘I would feel aggravated by X’. All these sub-scales were associated with the aspects of stigma which are prejudice, discrimination and ignorance, consequently allowing the researcher to investigate the levels of stigma. Once this was done participants were given a contact scale that was developed by Holmes and associates in order to investigate the familiarity with mental health problems. Questions such as ‘I have observed, in passing, a person I believe may have had a severe mental illness’ was asked (Corrigan, Canar, Holmes, Kubiak, & Williams, 1999). Finally, the shorter version of the culture scale that was developed by Triandis (1993) was finally used to assess the levels of individualism and collectivism cultural dimensions while focusing on the vertical- horizontal aspects of it as well. The Vertical-Horizontal Individualism-Collectivism Scale has 16 statements such as ‘I would do what would please my family even if I detested that activity’. The participants respond to the statements on a Likert Scale ranging from 1 (not at all) to 4 (always).
Design
The design of the study was independent groups design. The dependent variable was stigma levels and the independent variables were knowledge about mental health, familiarity and culture.
Procedure
Prior to the study, the questionnaires, consent form, information sheet and debriefing form were translated to Turkish by the researcher, to Greek by a Greek speaker and back-translated to English by independent. Once the agreement was reached on the translation the researcher obtained the ethical approval from Middlesex University of London. The researcher then set up an online survey using e-Surv, which is an online survey, programme commonly used by the researchers. The online survey initially included the information sheet and then the consent form for participants, which asked them to enter their name meaning that they consent to take part in the study. Once they completed filling the consent form they were asked to provide demographic information; age, gender, occupation and education level. They were also asked to provide their contact details; either email address or a phone number as the researcher then aims to carry out interviews with some of the participants. Once these were completed they were represented with two vignettes. One of these was about a man who had general life stress and the other one was about a man who had schizophrenia. They were then asked to complete a questionnaire assessing their knowledge in regards to these conditions. They then were represented with another vignette about a guy with schizophrenia and were required to complete the AQ-27 in relation to the vignette, which they have previously read. Once them completed AQ-27 they were required to complete the familiarity scale in order to assess how familiar they were with mental health problems. Finally, they completed the culture scale developed by Triandis (1993) assessing each of the two societies’ cultural structures. They took 15-25 minutes to complete the questionnaires. Upon completion of the scales they were represented with a debriefing sheet which included the researcher’s and the supervisory team’s contact details and a helpline contact number in case they wanted to seek help as the nature of the research was sensitive.
Findings
Stigma towards mental health problems was found to be existent in both Greek and Turkish Cypriot communities (See Figure 2). One-way ANOVA was carried out in order to assess the attitudes towards schizophrenia. Homogeneity of Variance was assumed due to a non-significant Levene’s test. The results showed that there was a significant difference between these two populations on their attitudes; F(1,98)=15.87, p<0.001, ηp2=.139.
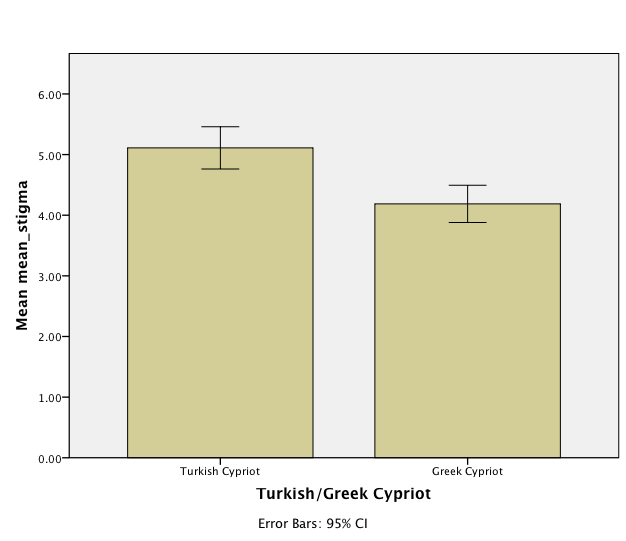
Turkish Cypriots had higher levels negative attitudes as opposed to Greek Cypriots (See Table 1). More detailed analysis has shown significant differences in anger, pity, coercion, help, segregation, fear and avoidance. Turkish Cypriots reported higher anger F(1,98)=93.57, p<0.001, fear F(1,98)=47.27, p=0.007, segregation F(1,98)=97.89, p<0.001, coercion F(1,98)-9.170, p=0.003. On the other hand, they significantly had lower levels of pity F(1,98)=88.51, p<0.001 and help F(1,98)=130.82, p<0.001.
There was not a significant difference between Turkish and Greek Cypriots for the control condition; F(1,98)=0.33, p=0.57 ηp2=.004. There was, however, a significant difference between Greek and Turkish Cypriots’ knowledge about schizophrenia; F(1,98)= 5.65, p=0.02 ηp2=.054. Although Turkish and Greek Cypriot’s knowledge did not significantly differ in regards to identification and the nature of the illness, they significantly differed in their perception of the treatment F(1,98)=54.349, p<0.001, ηp2=.051. Turkish Cypriots (52.9%) suggesting the treatment of schizophrenia “not being hard” as opposed to Greek Cypriots (95.9%) who suggested the illness being “very hard”. The two societies also differed in their perceptions about professional help F(1,98)=5.224 p=0.02, ηp2=.357. Turkish Cypriots were less likely to advice seeking professional help and significantly endorsed self-reliance (76.5%) more compared to Greek Cypriots who endorsed seeking professional help more (95.9). Furthermore, there was also a significant difference in advice which was given by the two population F(1,98)=115.669, p<0.001 ηp2=.541. Turkish Cypriots recommended reducing stress, speaking to close family as opposed to Greek Cypriots who highly endorsed seeking professional help for Schizophrenia.
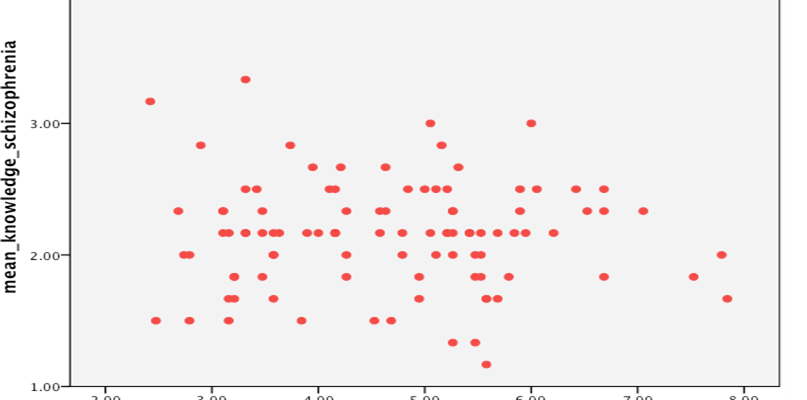
When looked at the relationship between knowledge and attitudes towards schizophrenia the correlational analysis showed weak but significant negative relationship; r(98)=-0.07, p=0.04 (See Figure 3).
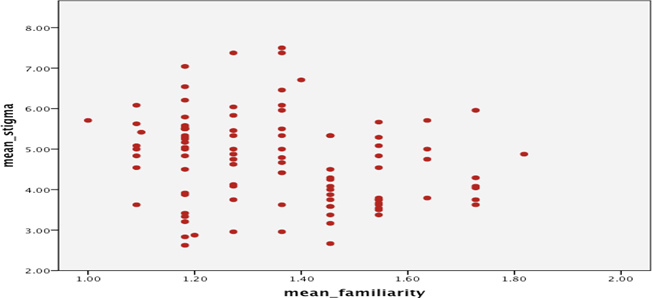
Furthermore, Greek and Turkish Cypriots significantly differed in their familiarity with mental health problems; F(1,98)=19.194, p=0.001 ηp2=.183. Greek Cypriots were significantly more familiar with mental health problems compared to Turkish Cypriots (See Table 1). Following a Pearson’s correlation was carried out in order to examine the relationship between stigma and familiarity. Results showed a negative significant relationship between these two variables; r(98)=-0.423, p=0.001 (See Figure 4).
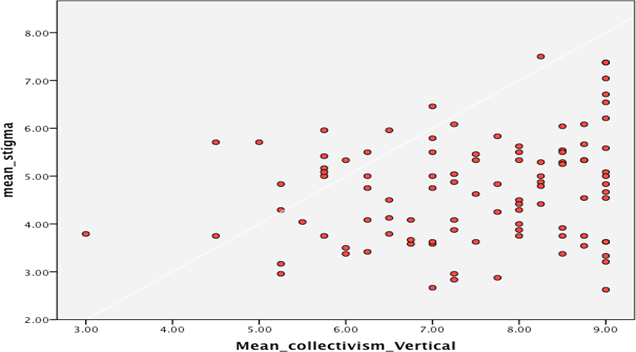
In addition to these cultural differences were also found amongst the two societies. Turkish Cypriots were significantly more vertical collectivist as compared to Greek Cypriots; F(1,98)=10.635, p=0.002 ηp2=.098. Pearson’s Correlation analysis also showed a significant positive relationship between vertical collectivism and stigma; r(98)=0.21, p=0.04 (See Figure 5).
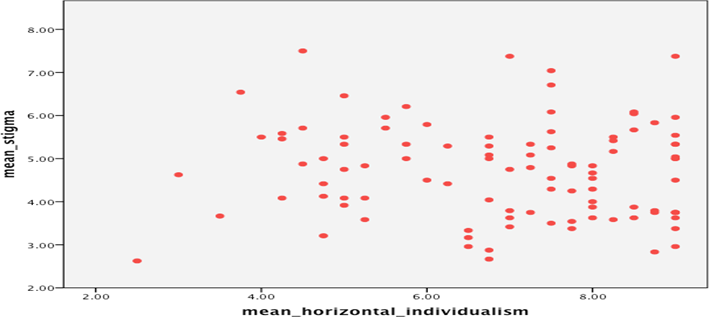
Furthermore, Greek Cypriots were significantly more horizontal individualist as opposed to Turkish Cypriots; F(1,98)=5.632, p=0.02 ηp2=.054. There was also, a negative non- significant relationship between horizontal individualism and stigma; r (98)=-0.01, p=0.5 (See Figure 6).
Conclusions
As expected, the results of this study showed that the Northern Cypriot participants reported significantly more negative attitudes. This was correlated with lack of knowledge about schizophrenia and familiarity as well as the more collectivist structure of the culture in the Northern side of the island.
Parallel to these findings knowledge, familiarity and cultural beliefs and values have been identified by the previus researchers as contributing factors to the stigma of mental illness (Evans-Lacko, Henderson, & Thornicroft, 2013; Stier & Hinshaw, 2007; Zartaloudi & Madianos, 2010; Papadapoulos, 2009; Cheon, 2012). Research that looked into the relationship between knowledge and stigma reported mixed findings. For example Leiderman, Vazquez, Berizzo, Bonifacio, Bruscoli, Capria, and Milev (2011) suggested that increased knowledge is not necessarily related to improved attitudes. Others such as Smith Reddy, Foster, Asbury and Brooks (2011), however, reported parallel findings with this study where increased knowledge lead to reduced negative attitudes consequently lower levels of stigma (Shyangwa, Singh, & Khandelwal, 2003; Byrne, 2000; Rusch, Angermeyer & Corrigan, 2005; Torrey, 2011). For example, Mino et al., (2000) at the final (5th) year medical training students report a higher levels of positive and accepting attitudes towards mental illness compared to a first year medical student. This was also supported in a study carried out in Turkey where the fifth year medical students were found to hold more positive attitudes compared to the second year students (Ay et al., 2006). These conflicting views may be due to knowledge alone not being enough to improve attitudes.
According to researchers such as Thornicroft, Brohan, Kassam and Lewis Holmes, 2008; and Arboleda-Florez and Stuart, 2012 suggested that improving public’s accurate knowledge helps reduce stigma towards mental health problems especially when it is combined with contact. A significant difference in regards to familiarity with mental illness was also found between Turkish and Greek Cypriots. Greek Cypriots were found to be more familiar with mental health problems as opposed to Turkish Cypriots. Consistent with the findings of this study many suggested that increased familiarity with mental illness reduces negative attitudes consequently stigma associated with these conditions. According to Corrigan, Green, Kubiak, Lundin and Penn (2001), both familiarity and social distance have been found to be significantly associated with mental illness stigma. According to them these constructs could be seen as interacting concepts that help describe mental illness stigma. This is because familiarity with mental health problems impacts on the stigma levels which also influences one’s desire to be socially distant from individuals with mental health problems (Corrigan, Green, Kubiak, Lundin, & Penn, 2001). Similarly, they also conducted a study in order to investigate the impact of familiarity on fear and social distance consequently stigma levels. They recruited 208 students who were required to complete a 21-Item Attitude Questionnaire developed by Reisenzein and a Level of Familiarity Scale developed by Holmes and associates. Their findings were parallel to this study. According to them those who were more familiar with mental health problems also had more knowledge and less stigmatizing attitudes towards individuals with these conditions. Furthermore, they also found that the discrimination levels were negatively correlated with familiarity.
Varying levels of familiarity and knowledge amongst the two societies may be due to the differences in their policies and regulations specifically for mental health. For example, in 2011 it was reported by WHO Mental Health Atlas that there are five-day treatment services in the Southern part specifically for mental health where as there is none in Northern side. Services available to mental health problems contribute to the reduction of stigma in the societies by increasing the awareness on mental health (WHO, 2003). Furthermore, the Southern part has a revised policy and regulation for mental health that was revised in 1997 after WHO regulations in regards to the care and treatment of those with mental health problems. This act is more concerned about the patients’ rights and integrative care of those with mental illness using multidisciplinary teams; lawyer, psychiatrists, psychologists and social workers. It also aims to improve the care to the European standards and integrate mental health with the community care, which in turn will further improve the mentally ill patients’ lives. On the other hand, the Northern side is still using the 1931 policy. In that policy mentally ill individuals are defined as “someone idiotic, mad and out of their healthy minds” (Republic of Northern Cyprus Mental Health Policy, 1931). This is very stigmatizing and may impact attitudes of the public. Anti-stigma campaigns have also been designed in the Southern part of the island aiming to increase awareness and knowledge about mental health which may contribute to the more favorable attitudes reported by the Greek Cypriot participants (Campaign, 2001). More research is needed to examine the direct influence of these factors on attitudes towards mental illness.
Finally, culture was also found to affect stigma associated with mental health problems. Although both cultures scored high in collectivism, Turkish Cypriots were found to be significantly more vertical collectivist. Findings from the previous studies reported varying levels of stigma amongst different cultural groups (Anglin Link, & Phelan, 2006; Rao, Kekwaletswe, Hosek, Martinez, & Rodriguez, 2007). According to Triandis (1993) in cultures that are more collectivist such as China the attitudes are more negative due to the emphasis on group harmony and togetherness, this is opposite to those whore are more individualist such as UK. In this study, it was found that although the more collectivist Turkish Cypriots were significantly more stigmatizing towards schizophrenia.
These findings could be explained using psycho-social framework (See Figure 1). According to this model individuals have experiences that include culture, familiarity and labeling which influences their perception about mental illness and mentally ill, this then helps form affect leading to emotional responses such as fear, anger and pity. In this study, the more collective structure of the Turkish Cypriot society combined with lack of knowledge and familiarity with mental health problems (experience) resulted in higher perception of dangerousness, which in turn resulted in more anger, fear and lower pity (affect). This has led to increased avoidance and discrimination of those with schizophrenia (behavioral response).
Although this study brings new findings in the field of mental illness stigma considering it’s the first comparison study ever to be conducted in Cyprus, it does have some limitations. Compared to the Southern Cypriots Northern Cypriots were slightly older and previous studies have found a link between age and stigmatizing attitudes towards mental illness; older generation reporting higher levels of stigma compared to the younger generation (Niwako, Yamawaki, Pulsipher, Moses, Rasmuse, & Ringger, 2011). In addition to this, most of the participants were educated to the higher level which might have influenced the findings. According to some researchers higher levels of education lead to higher tolerance towards mental illness consequently reduced negative attitudes (Girma, Emöller-Leimkühler, Müller, Dehning, Froeschl, & Tesfaye, 2014; Hannigan, 1999). Future research should, therefore, match participants in regards to their socio-economic status. Finally, it should be noted that the vignette used in this study for the attitude scale was about a person with schizophrenia, future research should focus on other mental health conditions as well in order to be able to get a better understanding of the attitudes towards different mental health problems. Despite these limitations, the findings of this study provide a valuable understanding of the stigmatization of schizophrenia in Cyprus. It also gives insight to public’s beliefs about schizophrenia and allows researchers for future development of interventions to reduce stigma.
In conclusion, level of stigma varies amongst the two societies due to the differences found between them in regards to knowledge, culture and familiarity. The joint anti-stigma campaigns are needed for the two societies to benefit from each-other and reduce stigma commonly. Furthermore, interventions should also be sensitive to the collective structure of the Northern Cypriots.
Acknowledgements
The author(s) declare that there is no conflict of interest.
References
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social. Behaviour. Englewood Cliffs, NJ: Prentice-Hall.
Angermeyer, M. C., & Matschinger, H. (2003). The stigma of mental illness: effects of labelling on public attitudes towards people with mental disorder. Acta Psychiatrica Scandinavica, 108(4), 304-309. DOI:
Anglin, D., Link, B., & Phelan, J. (2006). Racial differences in stigmatizing attitudes toward people with mental illness. Psychiatric Services, 57(6), 857-862. DOI:
Arboleda-Florez J, Stuart H: From sin to science: fighting the stigmatization of mental illnesses. Can J Psychiatry 2012, 57(8):457-463. DOI:
Arkar, H., & Eker, D. (1994). Effect of psychiatric labels on attitudes toward mental illness in a Turkish sample. International Journal of Social Psychiatry, 40(3), 205-213. DOI:
Alexander, L., & Link, B. (2003). The impact of contact on stigmatizing attitudes toward people with mental illness. Journal of Mental Health, 12(3), 271-289. DOI:
Alonso, J., Angermeyer, M. C., Bernert, S., Bruffaerts, R., Brugha, T. S., Bryson, H., & Vollebergh, W. A. M. (2004). Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica, 109(s420), 21-27. DOI:
Avruch, K. (1998). Culture and conflict resolution (Vol. 31). US Institute of Peace Press.
Baumann, A. E. (2007). Stigmatization, social distance and exclusion because of mental illness: the individual with mental illness as a'stranger'. International Review of Psychiatry, 19(2), 131-135. DOI:
Boatswain, T. (2005). A Traveller's History of Cyprus. Interlink Books. Bryant, Rebecca and Papadakis, Yiannis, eds (2012) Cyprus and the politics of memory: history, community and conflict International library of twentieth century history.
Byrne, P. (2001). Psychiatric stigma. The British Journal of Psychiatry, 178(3), 281-284. DOI:
Campaign, A. (2001). Results of a Global Advocacy Campaign.
Cheon, B. K., & Chiao, J. Y. (2012). Cultural variation in implicit mental illness stigma. Journal of cross-cultural psychology, 43(7), 1058-1062. DOI:
Cooper-Patrick, L., Gallo, J. J., Gonzales, J. J., Vu, H. T., Powe, N. R., Nelson, C., & Ford, D. E. (1999). Race, gender, and partnership in the patient-physician relationship. Jama, 282(6), 583-589. DOI:
Corrigan, P. W. (2000). Mental health stigma as social attribution: Implications for research methods and attitude change. Clinical Psychology: Science and Practice, 7(1), 48-67. DOI:
Corrigan, P. W., Edwards, A. B., Green, A., Diwan, S. L., & Penn, D. L. (2001). Prejudice, social distance, and familiarity with mental illness. Schizophrenia bulletin, 27(2), 219. DOI:
Corrigan, P., Markowitz, F. E., Watson, A., Rowan, D., & Kubiak, M. A. (2003). An attribution model of public discrimination towards persons with mental illness. Journal of Health and Social Behavior, 162-179. DOI:
Corrigan, P. W., Green, A., Lundin, R., Kubiak, M. A., & Penn, D. L. (2001). Familiarity with and social distance from people who have serious mental illness. Psychiatric services, 52(7), 953-958. DOI:
Economou, M., Richardson, C., Gramandani, C., Stalikas, A., & Stefanis, C. (2009). Knowledge about schizophrenia and attitudes towards people with schizophrenia in Greece. International Journal of Social Psychiatry, 55(4), 361-371. DOI:
Eker, D. (1989). Attitudes toward mental illness: Recognition, desired social distance, expected burden and negative influence on mental health among Turkish freshmen. Social Psychiatry and Psychiatric Epidemiology, 24(3), 146-150. DOI:
El-Badri, S., & Mellsop, G. (2007). Stigma and quality of life as experienced by people with mental illness. Australasian Psychiatry, 15(3), 195-200. DOI:
Evans-Lacko, S., Henderson, C., & Thornicroft, G. (2013). Public knowledge, attitudes and behaviour regarding people with mental illness in England 2009-2012. The British Journal of Psychiatry, 202(s55), s51- s57. DOI:
Fabrega Jr, H. (1991). Psychiatric stigma in non-Western societies. Comprehensive psychiatry, 32(6), 534-551. DOI:
Gaebel, W., Baumann, A., Witte, A. M., & Zaeske, H. (2002). Public attitudes towards people with mental illness in six German cities. European archives of psychiatry and clinical neuroscience, 252(6), 278- 287. DOI:
Girma, E., Möller-Leimkühler, A. M., Müller, N., Dehning, S., Froeschl, G., & Tesfaye, M. (2014). Public stigma against family members of people with mental illness: findings from the Gilgel Gibe Field Research Center (GGFRC), Southwest Ethiopia. BMC international health and human rights, 14(1), 2. DOI:
Halter, M. J. (2008). Perceived characteristics of psychiatric nurses: Stigma by association. Archives of psychiatric nursing, 22(1), 20-26. DOI:
Hannigan, B. (1999). Mental health care in the community: An analysis of contemporary public attitudes towards, and public representations of, mental illness. Journal of Mental Health, 8(5), 431-440. DOI:
Hampton, N. Z., & Sharp, S. E. (2014). Shame-Focused Attitudes Toward Mental Health Problems The Role of Gender and Culture. Rehabilitation Counseling Bulletin, 57(3), 170-181. DOI:
Heider, J. (1958). The psychology of interpersonal relations. New York: Wiley. DOI:
Hinshaw, S. P., & Stier, A. (2008). Stigma as related to mental disorders. Annu. Rev. Clin. Psychol., 4, 367-393. DOI:
Jorm, A. F. (2000). Mental health literacy Public knowledge and beliefs about mental disorders. The British Journal of Psychiatry, 177(5), 396-401. DOI:
Jorm, A. F., & Reavley, N. J. (2012). Changes in psychological distress in Australian adults between 1995 and 2011. Australian and New Zealand Journal of Psychiatry, 46(4), 352-356. DOI:
Kim, D., Kim, C. H., Moon, J. I., Chung, Y. G., Chang, M. Y., Han, B. S., & Kim, K. S. (2009). Generation of human induced pluripotent stem cells by direct delivery of reprogramming proteins. Cell stem cell, 4(6), 472. DOI:
Kirmayer, L. J. (2001). Cultural variations in the clinical presentation of depression and anxiety: implications for diagnosis and treatment. Journal of Clinical Psychiatry, 62, 22-30.
Kroeber, A. L., & Kluckhohn, C. (1952). Culture: A critical review of concepts and definitions. Papers. Peabody Museum of Archaeology & Ethnology, Harvard University.
Leiderman, E., Vazquez, G., Berizzo, C., Bonifacio, A., Bruscoli, N., Capria, J. I., Milev, R. (2011). Public knowledge, beliefs and attitudes towards patients with schizophrenia: Buenos Aires. Social Psychiatry and Psychiatric Epidemiology, 46(4), 281-290. DOI:
Link, B. G., & Phelan, J. C. (2001). Conceptualizing stigma. Annual review of Sociology, 363-385. DOI:
Littlewood, R. (1998). Cultural variation in the stigmatisation of mental illness. Lancet, 352, 1056–1057. DOI:
Madianos, M. G., Madianou, D., Vlachonikolis, J., & Stefanis, C. N. (1987). Attitudes towards mental illness in the Athens area: implications for community mental health intervention. Acta Psychiatrica Scandinavica, 75(2), 158-165. DOI:
Marwaha, S., & Johnson, S. (2005). Views and experiences of employment among people with psychosis: a qualitative descriptive study. International Journal of Social Psychiatry, 51(4), 302-316. DOI:
Mellor, D., Carne, L., Shen, Y. C., McCabe, M., & Wang, L. (2013). Stigma toward mental illness: a cross-cultural comparison of Taiwanese, Chinese immigrants to Australia and Anglo- Australians, Journal of cross-cultural psychology, vol. 44(3), 352-364. DOI:
Mojtabai, R. (2010). Mental illness stigma and willingness to seek mental health care in the European Union. Social psychiatry and psychiatric epidemiology, 45(7), 705-712. DOI:
Nee, C., & Witt, C. (2013). Public perceptions of risk in criminality: The effects of mental illness and social disadvantage. Psychiatry research, 209(3), 675-683. DOI:
Norman, R. M., Sorrentino, R. M., Gawronski, B., Szeto, A. C., Ye, Y., & Windell, D. (2010). Attitudes and physical distance to an individual with schizophrenia: the moderating effect of self-transcendent values. Social psychiatry and psychiatric epidemiology, 45(7), 751-758. DOI:
Panayiotopoulos, C., Pavlakis, A., & Apostolou, M. (2012). Improving mental health services through the measurement of attitudes and knowledge of mental health professionals and the general population in Cyprus. Int J Ment Heal, 41(4), 29-46. DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.