
Factors Affecting Self-Reported Pain in Children Receiving Dental Treatment

Abstract
The aim of the current study is to investigate the ability of self-reported pain tools to help dentists during pederatic patient managment and to determine the effect of different interpersonal and treatment variables as well as the level of dental anxiety on a child’s self-report pain and change after dental injection procedure. A randomized multicenter two arms clinical trial was conducted with a total of fifty children who were enrolled and divded into two groups (n = 25). The mean Group I age was 7.99 ± 0.81 and was randomly selected from pedodontics clinics at the faculty of dentistry (October 6 university, Egypt); Group II’s mean age was 7.73 ± 0.60 and was randomly selected from outpatient Tanta governmental hospitals. The tools used in the current research were personal interview, dental operator questionnaire, Venham picture test, Visual analogue scale and Wong Baker faces pain scale. İt was concluded that self reported pain in children is a relevant tool that can be used successfully for assessment of dental pain which can help dental practitioners deliver effective treatment. The most powerful factors which influence self-reported pain are age, previous positive dental experience and level of dental anxiety. This study will enable dental practioners to empathise with and deal successfully with children undergoing dental procedures.
Introduction
It is widely accepted in the area of paediatric dentistry that children’s dental fear and anxiety (DFA) and dental behavioural management problems (DMBP) often create barriers to successful treatment. (Townend et al., 2000). Acute pain is one of the most common adverse stimuli experienced by children, occurring as a result of injury, illness and medical procedures. If a child's pain is not treated quickly and effectively, it can have long-term physical and psychological sequelae. Long-term consequences may include anticipatory anxiety during future procedures, a lowering of the pain threshold and sensitization to future pain, reduced effectiveness of analgesics and increased analgesic requirements for subsequent procedures (Wong et al., 2012a).
However, it is known that the pain sensation is not necessarily dependent on tissue damage. In dentistry, it may also be initiated by conditioned stimuli such as the sound of the drill or the use of the needle during local anesthesia (Wong et al., 2012b). Furthermore, pain related to dental treatment has been shown to be an important factor in the etiology of dental fear. According to Roberts, painful dental treatments can cause fear, whereas fear and anxiety can increase the amount of perceived pain (Welbury et al., 2012). This is particularly important in pediatric dentistry, as it is known that dental anxiety and fear are related to negative or traumatic dental experiences during childhood (de Menezes Abreu et al., 2011).
Pain is a subjective experience, based on an individual’s perspective which implies that verification becomes a problem. Verification would require an objective observation of the phenomenon. The appropriate management of pain relies on the ability to accurately assess the extent of pain using a valid tool. Self-report is regarded as the primary source for assessment because pain is primarily an internal experience, and many children 4 years and older are able to provide meaningful reports of pain intensity when using the appropriate tools (von Baeyer, 2006; Srouji et al., 2010).
Self-report measures have often been underutilized in assessing children’s pain. They can be used in conjunction with observer reports of pain and can provide a valuable indication of treatment outcome in both clinical and research contexts.
The pain intensity scales most commonly used with children include faces scales, numerical rating scales, visual analogue scales and others. Faces scales and visual analogue scales are subjective scales that measure pain intensity in children. Accordingly, pain management is improved when pain is regularly and reliably measured (von Baeyer, 2009).
Numerous studies have shown that dental anxiety is correlated with fear of pain and previous negative experiences in the dental setting (Vassend, 1993; De Jongh et al., 2006). Dental anxiety often originates in childhood (51%) or adolescence (22%) (Locker, 1999). The onset of anxiety in childhood may result from a conditioning process, either through personal negative experience or through modelling by parents or peers. Socioeconomic and cultural factors have been shown to influence anxiety and behaviour during dental treatment.
General emotional status is also an etiological factor, and some temperaments in children, such as shyness and negative emotionality, may place them at risk of developing dental anxiety. Moreover, associated medical conditions or cognitive deficiency put children at risk of experiencing difficulty in coping with the dental situation (Nicolas et al., 2010).
It is accepted that children’s reactions are strongly affected by situational factors such as the information provided, their coping ability, their anticipatory anxiety and their previous experience (Versloot et al., 2008). For a pedodontist to deliver effective treatment, a detailed understanding of the factors influencing children’s anxiety, fear and pain perception is important in planning methods to help the child cope with treatment procedures.
Problem Statement
Pain assessment can have several functions. At minimum, it can be used to indicate the need for intervention, as well as to evaluate the effectiveness of treatments designed to reduce pain. Also, pain assessment is necessary to determine the associations between levels of pain and other variables. This explicative type of research, typically conducted using correlational methods, is useful for understanding how other factors are related to pain and for constructing theoretical models of pain. Some correlated variables simply occur together with pain, while others may have a causal influence. It is important to evaluate the relationship between the pre-procedural anxiety and the child’s self-reported pain in consequent events to determine the related effects of treatment approaches, interpersonal variables such as the child’s age, gender, previous dental experience and level of dental anxiety as well as the injection site on the reported pain ratings.
Research Question
This study is guided by the following question; “What are the factors affecting the child dental patient in coping with dental procedures?”
Purpose of the Study
The aim of this study is to determine the effect of different interpersonal and treatment variables and the level of dental anxiety on the child’s self-report pain and assess the changes that occur in the child’s pain after dental injections.
Research Design and Procedure
Study design
A non-experimental randomized multicenter two arms clinical trial, analytical design was used for this study.
Study settings
- Pediatric Dentistry Department, Faculty of Dentistry, 6 October University.
- Tanta Governmental Hospital.
Study Sample
Fifty children were recruited for this study. The study sample was divided into two equal groups (25 each), according to the geographic location of dental treatment facilities. Written consent was obtained from the parents.
- Group I: Patients were randomly selected from the outpatient clinic and were treated by the dental operator in the Pediatric Dentistry Department, Faculty of Dentistry, 6 October University.
- Group II: Patients were randomly selected from the outpatient clinic and were treated by the dental operator in the Tanta Governmental Hospital dental clinic.
The criteria for the selection of children were:
- Children aged from 7-12 years
- Children in need of restoration of their primary molars with treatment requiring local anesthesia.
- Children with no physical or mental disabilities.
- Informed consent for ethical consideration
Study tools
- Patient chart
- The Venham Picture Test (VPT).
- The Visual Analogue scale (VAS).
- The Wong Baker Faces Pain Scale (WBFPS).
- Dental operator questionnaire.
Methods
A chart was designed to record the patients' basic demographic data including age, gender, previous dental treatment and type of service done.
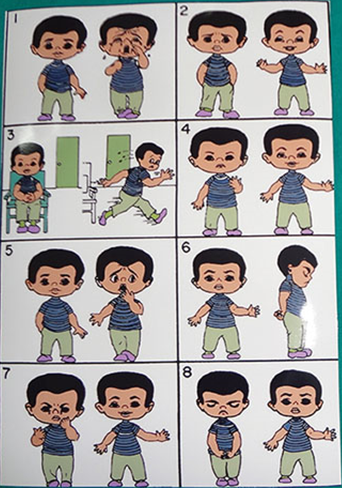
The Venham Picture Test (VPT)
Before the dental injection, the level of anxiety was predicted using the Venham Picture Test. The test is easy to administer and score, as it consists of eight cards with pictures of children in various dental situations. There are two figures on each card, one in which a child appears happy and the other one in which he looks distressed. The children were asked to point at the figure that represented their feelings at that moment. A score was recorded for each card when the "high fear" picture was selected and summed to give total out of eight. Higher scores indicate greater fear.
Dental Injection
Nonpharmacologic behavior management techniques are routinely performed; all dental injections were given after application of topical anesthesia.
Self-reported pain
Following the dental injection which was performed by the dental operator in each dental setting and before starting the restorative procedure, each child was asked to point out the level of pain using the following scales:
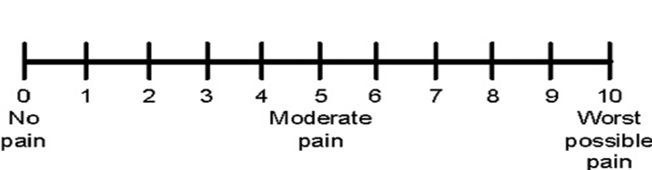
The Visual Analogue scale (VAS)
A simple assessment tool consisting of a 10 cm line with 0 on one end, representing no pain, and 10 on the other, representing the worst pain. Children were asked to make a mark on the line that represented their level of perceived pain intensity.
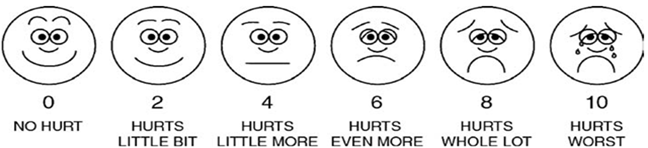
Wong Baker Faces Scale (WBFS)
The scale shows a series of faces ranging from a happy face at 0-"No hurt" to a crying face at 10-"Hurts worst". The children had to choose the face that best described how they felt.
Dental operator questionnaire
Following the completion of the restorative treatment, the dental operators filled out a questionnaire which included the following items.
- Dental operator: General practitioner or pediatric dentist
- Years in current post and average number of patients treated per day
- Place of dental treatment
- Waiting time and treatment time
- Type of dental injection (infiltration or nerve block)
Statistical analysis
Data were collected and tabulated using Microsost Excel and all statistical analysis was performed using
SPSS v.18.0 (IBM Corp., Armonk, NY, USA). A p-value ≤ 0.05 was considered significant for all statistical tests.
Findings
The age in Group I ranged between 7 to 10 years (mean = 7.99±0.81 years), while the age in Group II ranged from 7 to 9.6 years (mean = 7.73±0.60 years ). In terms of gender, Group I comprised 15 males and 10 females while Group II comprised 13 males and 12 females. The analysis showed that in relation to Age, Gender or Previous dental experience there were no signficant differences in distribution between the two groups (paired t-test for age; Chi Square test and Monte Carlo test for pervious dental experience, p=0.089,0.569, 0.556 respectively).
As for the child anxiety level before dental injections using the Venham Picture Test (VPT) the children’s anxiety in Group I ranged from 0 to 8 ( mean = 1.52 ± 2.26) while in Group II, it ranged from 0 to 7 (mean = 1.72 ± 1.96) (p=0.208) Meanwhile, regarding the type of dental injection used, there was a significant difference between the two groups where 19 children had Infliration anathestia and 6 children had Nerve block in Group I while 10 children had Infliration anathestia and 10 children had nerve block in Group II (Wilcoxon signed-rank test, p= 0.01).
There was no significant difference in the children’s self-reported pain between the two groups (using the Visual Analog Scale (VAS) where self reported pain ranged from 0 to 7 (mean =2.8±2.06) for Group I and from 0 to 10 (mean =3.24±3.8) for Group II (p=0.55). This was echoed in the Wong Baker Faces Scale (WBFS) where self reported pain ranged from 0 to 3 (mean =1.4±1) for Group I and from 0 to 5 (mean =1.96±1.74) for Group II (p=0.536). There was no significant difference between the two groups in treatment time (p ˂ 0.469) or waiting time (p ˂ 0.001). (Wilcoxon signed-rank test for self-reported pain, paired t-test for treatment and waiting time).
As for the personal data of the dental operator, there was no significant difference (paired t-test) in age (p˂ 0.213), gender (p˂0.136) or years since graduation (p˂0.503). The only significant difference was seen between the two groups in number of patients treated per day (p˂0.001). Correlation was analysed between self-reported pain scores using (VAS) and the child’s age, dental anxiety level (VPT) and waiting time. The two groups showed an inverse correlation between self-reported pain scores (VAS) and the child’s age in both group, but no signoficance was found (Spearman's rank correlation coefficient =-0.1 and -0.2; p=0.220, p= 0.339) respectively. A positive correlation was found between self-reported pain scores (VAS) and dental anxiety scores (VPT). The correlation was significant in Group I (Spearman's rank correlation coefficient = 0.56 ; p = 0.004), but not significant in Group II (Spearman's rank correlation coefficient = 0.1 p = 0.292). A positive correlation was found between self-reported pain scores (VAS) and waiting time in Group I while an inverse correlation was seen in Group II. However, both correlations were not significant (Spearman's rank correlation coefficient = 0.1 and -0.2 ; p = 0.254, p =0.383) respectively.
As for the correlation between self-reported pain scores using (WBFPS) and the child’s age, dental anxiety level (VPT) and waiting time, an inverse correlation was found in both groups between self-reported pain scores (WBFPS) and the child’s age. Again, the correlation was not significant (Spearman's rank correlation coefficient =0.42 and 0.21 p=0.189, p=0.755) respectively. A positive correlation between self-reported pain scores (WBFPS) and dental anxiety scores (VPT) was found. The correlation was significant in Group I ( R=0.55 p= 0.001), but not in Group II (R=0.21 p=0.257). A positive correlation was found between self-reported pain scores (WBFPS) and waiting time in Group I while an inverse correlation was seen in Group II. However, both correlations were not significant (R=0.1,-0.12 p=0.388, p=0.159) respectively.
Relationship between self-reported pain scores using VAS and the child’s gender
- Group I
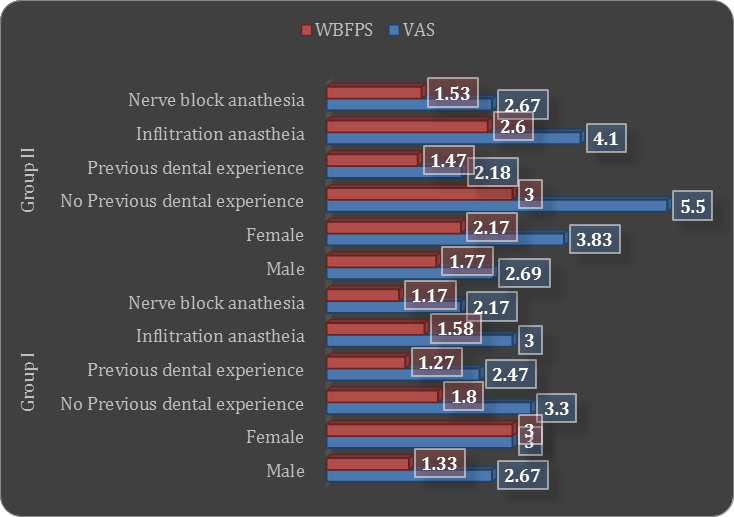
Male children self-reported pain scores ranged between 0 to 7 (mean = 2.67 ± 2.32), while female children self-reported pain scores ranged between 0 to 6 (mean = 3.00 ± 1.70). No significant difference was found in the self-reported pain scores between males and females. (Wilcoxon signed-rank test ; p = 0.435)
- Group II
Male children self-reported pain scores ranged between 0 to 10 (mean = 2.69 ± 3.64), while female children self-reported pain scores ranged between 0 to 10 (mean = 3.83 ± 4.04). No significant difference was found in self-reported pain scores between males and females. (Wilcoxon signed-rank test; p = 0.416).
Relationship between self-reported pain scores using WBFPS and the child’s gender
- Group I
Male children self-reported pain scores ranged between 0 to 3 (mean = 1.33 ± 1.11), while female children self-reported pain scores ranged between 1 to 3 (mean = 3.00 ± 1.70). No significant difference was found in self-reported pain scores between males and females. (Wilcoxon signed-rank test; p = 0.705)
- Group II
Male children self-reported pain scores ranged between 0 to 5 (mean = 1.77 ± 1.64), while female children self-reported pain scores ranged between 0 to 5 (mean = 2.17 ± 1.90). There was no significant difference in self-reported pain scores between males and females. (Wilcoxon signed-rank test , p = 0.028).
Relationship between self-reported pain scores using VAS and the previous dental experience
- Group I
Children who had no previous dental experiance self reported pain scores ranging from 1 to 6 (mean = 3.30 ± 2.11) whereas children having previous dental experience self reported pain scores ranging from 0 to 7 (mean = 2.47±2.03) (Wilcoxon signed-rank test , p = 0.352).
- Group II
Children who had no previous dental experience self reported pain scores ranging from 0 to 10 (mean = 5.50 ± 4.47) whereas children having previous dental experience self reported pain scores ranging from 0 to 10 (mean = 2.18 ± 3.03) (Wilcoxon signed-rank test , p = 0.099).
Relationship between self reported pain scores using WBFPS and the previous dental experience
- Group I
Children who had no previous dental experience self reported pain scores ranging from 0 to 3 (mean = 1.8 ± 1.14) whereas children having previous dental experience self reported pain scores ranging from 0 to 3 (mean = 1.27±0.88) (Wilcoxon signed-rank test. p = 0.245).
- Group II
Children who had no previous dental experience self reported pain scores ranging from 0 to 5 (mean = 3 ± 1.85) whereas children having previous dental experience self reported pain scores ranging from 0 to 5 (mean = 1.47 ± 1.5) (Wilcoxon signed-rank test , p = 0.053).
Relationship between self-reported pain scores using VAS and the type of dental injection
- Group I
Children who received inflitration anasthesia self reported pain scores ranging from 0 to 7 (mean = 3 ± 2.91) whereas children who received nerve block anasthesia self reported pain scores ranging from 0 to 4 (mean = 2.17±1.60) (Wilcoxon signed-rank test , p = 0.439).
- Group II
Children who recieved inflitration anasthesia self reported pain scores ranging from 0 to10 (mean = 4.10 ± 4.12) whereas children receiving nerve block anasthesia self reported pain scores ranging from 0 to 10 (mean = 2.67 ± 3.60) (Wilcoxon signed-rank test , p = 0.458).
Relationship between self-reported pain scores using WBFPS and the type of dental injection
- Group I
Children who received inflitration anasthesia self reported pain scores ranging from 0 to 3 (mean = 1.58 ± 1.07) whereas children receiving nerve block anasthesia self reported pain scores ranging from 0 to 2 (mean 1.17 ± 0.75) (Wilcoxon signed-rank test, p = 0.424).
- Group II
Children who received inflitration anasthesia self reported pain scores ranging from 0 to5(mean = 2.60 ± 1.90) whereas children receiving nerve block anathesia self reportd pain scores ranging from 0 to 5 (mean 1.53 ± 1.55) (Wilcoxon signed-rank test , p = 0.157).
Conclusion
Based on the results of the present study, it can be concluded that the most influential factors on the self-reported pain among a group of Egyptian children were the child’s age, previous dental experience and level of dental anxiety. The WBFPS proved to be more valuable, comprehensible and easier to use by the children and gave better results than the VAS. These results would encourage the general practitioner to use the proper behavior management techniques in modifying the child’s pain response. Assessment of pain and anxiety level of children before starting treatment proved to be successfully applied and can help improve the quality of delivered treatment through the selection of a proper approach of pain management.
Implications
The current research has highlighted that self reported pain in children is a relevant tool that can be used sucessfully to evaluate, understand and successfully manage the factors related to children’s pain. Managing children’s pain successfully has long term consequences for their perception of the level of pain related to receiving dental treatment. This perception will influence their outlook, either postively or negatively, to dental practitioners in general and to dental procedures in particular and since frequent dental visits are important to maintaning good dental health, this study has far reaching implications for both dental practitioners and children’s motivation to get adequate dental care.
Acknowledgements
The author(s) declare that there is no conflict of interest.
References
Abu‐Saad, H. H., & Hamers, J. P. (1997). Decision‐making and paediatric pain: a review. Journal of Advanced Nursing, 26(5), 946-952. DOI:
Chapman, H. R., & Kirby-Turner, N. (2002). Visual/verbal analogue scales: examples of brief assessment methods to aid management of child and adult patients in clinical practice. British dental journal, 193(8), 447-450. DOI:
De Jongh, A., Fransen, J., Oosterink-Wubbe, F., & Aartman, I. (2006). Psychological trauma exposure and trauma symptoms among individuals with high and low levels of dental anxiety. European journal of oral sciences, 114(4), 286-292. DOI:
De Menezes Abreu, D. M., Leal, S. C., Mulder, J., & Frencken, J. E. (2011). Pain experience after conventional, atraumatic, and ultraconservative restorative treatments in 6‐to 7‐yr‐old children. European journal of oral sciences, 119(2), 163-168. DOI:
Locker, D., Liddell, A., Dempster, L., & Shapiro, D. (1999). Age of onset of dental anxiety. Journal of dental research, 78(3), 790-796. DOI:
Nicolas, E., Bessadet, M., Collado, V., Carrasco, P., Rogerleroi, V., & Hennequin, M. (2010). Factors affecting dental fear in French children aged 5–12 years. International Journal of Paediatric Dentistry, 20(5), 366-373. DOI:
Ram, D., & Peretz, B. (2000). Reactions of children to maxillary infiltration and mandibular block injections. Pediatric dentistry, 23(4), 343-346.
Srouji, R., Ratnapalan, S., & Schneeweiss, S. (2010). Pain in children: assessment and nonpharmacological management. International Journal of Pediatrics. DOI:
Townend, E., Dimigen, G., & Fung, D. (2000). A clinical study of child dental anxiety. Behaviour research and therapy, 38(1), 31-46. DOI:
Vassend, O. (1993). Anxiety, pain and discomfort associated with dental treatment. Behaviour research and therapy, 31(7), 659-666. DOI:
Venham, L. L. (1978). The effect of mother's presence of child's response to dental treatment. ASDC journal of dentistry for children, 46(3), 219-225.
Versloot, J., Veerkamp, J. S., & Hoogstraten, J. (2008). Children’s self-reported pain at the dentist. Pain, 137(2), 389-394. DOI:
Von Baeyer, C. L. (2006). Children’s self-reports of pain intensity: scale selection, limitations and interpretation. Pain Research and Management, 11(3), 157-162. DOI:
von Baeyer, C. L., Spagrud, L. J., McCormick, J. C., Choo, E., Neville, K., & Connelly, M. A. (2009). Three new datasets supporting use of the Numerical Rating Scale (NRS-11) for children’s self-reports of pain intensity. PAIN, 143(3), 223-227. DOI:
Welbury, R., Duggal, M. S., & Hosey, M. T. (Eds.). (2012). Paediatric dentistry. OUP Oxford. DOI:
Wong, C., Lau, E., Palozzi, L., & Campbell, F. (2012a). Pain management in children: Part 1—Pain assessment tools and a brief review of nonpharmacological and pharmacological treatment options. Canadian Pharmacists Journal/Revue des Pharmaciens du Canada, 145(5), 222-225. DOI:
Wong, C., Lau, E., Palozzi, L., & Campbell, F. (2012b). Pain management in children: Part 2—A transition from codeine to morphine for moderate to severe pain in children. Canadian Pharmacists Journal/Revue des Pharmaciens du Canada, 145(6), 276 - 279. DOI:
Wong, D. L., & Baker, C. M. (2001). Smiling face as anchor for pain intensity scales. Pain, 89(2-3), 295-297. DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.