
Self-Harming Behavior And Its Relation With Previous Psychological or Psychiatric Care

Abstract
The study was realized in cooperation with grant support: MUNI/A/0790/2012 "Verifying the psychometric properties of diagnostic tools for screening the incidence and forms of self-harm among school children". This study explores self-harming behavior among adolescents (12-15 years old) and its relation with previous psychological or psychiatric care. There is a connection to the process occurrence type of self-harm between adolescents who have been or are in psychological or psychiatric care and those who were never been. The results can spread our knowledge about self-harm behavior, which is very common teenage phenomenon. Furthermore, it can be used to specify the support for adolescents who do self-harm. In accordance with the research objectives were quantitative, exploratory data, in a one-shot cross-sectional survey using self-report measures. Our sample was 1110 adolescents between 12 to 15 years old. In our sample were 84 adolescents who do or did self-harm. The methods for measuring self-harm included the Self-Harm Inventory (SHI; Sansone, Sansone, & Wiederman, 1995). The main differences were found in occurrence of self-harm behavior between children who have never been in psychological or psychiatric care (20%) and the others (40%). Small differences were found also in different type of self-harm behavior. On the other hand we did not find differences in the self-harm process. There are differences between those adolescents who have never been in psychological or psychiatric care and the others. We hope that the results of this study could help to understand the self-harming behavior, which is currently spreading among adolescents. It could be a useful guide for those, who are working with the youth.
Keywords: Self harm, Non-suicidal self ınjury, adolescents
Introduction
Self-harm, in recent years, has become a widespread phenomenon among adolescents. We have been dealing with this topic since 2011 and thus we reflect the need to expand the professional knowledge of the specifics and context of this phenomenon. Our study deals with self-harm behavior among adolescents aged 12-15 years in the context of their previous or current experience with professional psychological or psychiatric care. The study was realized with the financial support of MUNI/A/0790/2012 called "Verifying the psychometric properties of diagnostic tools for screening the incidence and forms of self-harm among school children".
Problem Statement
The first step is to define what in our study we consider self-injurious behavior. We respect the current theoretical concept that shows self-harm behavior as a direct and deliberate act of self- harming without any direct intent to die (Bartošová, 2014; Lieberman, 2004; Favazza 1998). Far more confusing is the use of terminology and classification of self-injurious behavior. We can encounter the terms as deliberate self-harm - DSH, self-harm, self-destructive behavior, automutilation (Krieglová, 2008). In some publications we can also find an identification of self- harm with a particular way of its execution - self-cutting, self-wounding, self-poisoning, delicate cutting (Krieglová, 2008; Platznerová, 2009). There are also expanding concepts such as self- injourious thoughts and behavior (Janis & Nock 2008) and RSM - repetitive-self-mutilation syndrome (Lieberman, 2004). Currently, there is also often used the term NSSI - nonsuicidal behavior that is mentioned in the new DSM V as a separate category. It is also necessary to understand the difference between self-harm behavior and suicide attempts. According to recent research, it is possible to trace differences in impulsivity (Carli et al., 2010), during the first attempts (Bertolote & Fleischmann, 2002). There is no denying that both phenomena may have some aspects similar or even identical but they cannot be equated. We will use the term “self-harm behavior” for our purposes as it can be used for various types of self- injurious behavior.
Although there are many types of self-harm behavior described in literature, for our purposes we used the classification of its types based on the questionnaire SHI - Self-Harm Inventory (Sansone, Sansone, & Wiederman, 1995), which we have used for the exploration of the issue. There were several exceptions of self-harm behavior that were thus excluded because they did not correspond with the age group of our respondents.
It is clear, from the theoretical discussion, that self-harm behavior can begin at any age but the most common occurrence is found in adolescents aged 12-15 years (Favazza, 1987). The results of foreign studies (Lieberman, 2004; Izutsu et al., 2006; Kvernmo & Rosenvinge, 2009; Whitlock, 2010) confirm that the age of the first self-harm attempt can be found around the 12th year of age.
Self-harm behavior is a phenomenon evolving from many factors and one of them is undoubtedly the resilience of an individual. In the earlier studies, self-harm behavior was seen only as one of the symptoms of various mental disorders, of which the extreme type of emotionally unstable personality disorder has the largest representation (Suyemoto, 1998; Evren & Evren, 2005; Messer et al., 2008). Furthermore, self-harm behavior is a frequent part of obsessive compulsive disorder, primarily as a ritual leading to release tension and getting a sense of control (Favazza, 1998; Messer et al, 2008).
Suyemoto (1998) dealt with a summary of theoretical concepts affecting self-harm behavior in his review study. Here he refers to the six models of self-harm behavior that seeks to explain its function. It is an environmental model, anti-suicidal model, sexual model, model of affect regulation, dissociative and borderline model. Dissociation is very often described as a part of self- harming act by patients. Himber (1994) notes, that self-harming can also cause dissociative state.
Skegg (2005) in his work reveals the concept of long-term and short-term factors that may cause the formation and development of self-harm behavior. For long-term factors can be mentioned separation or loss of a loved one, abuse in all forms, inappropriate access of nurses and social workers, permanent personality traits or mental illness. Short-term factors include various stressful situations, partner or family disagreements, substance abuse, lack of social supports, worsening of symptoms.
One of the characteristics of self-harm behavior is its cyclic repetition. Chapman et al. (2006) highlights this factor in his model Experimential avoidance model (EAM) of deliberate-self harm. It is therefore necessary to separate those teens who are only experimental users and those who have had some experience of self-harming.
It is therefore evident that self-harm behavior is not necessarily linked to mental illness and may thus also affect people who objectively at the moment do not suffer from other mental diseases. Currently, a great emphasis is placed on the issue of social imitation in the self-harm behavior among adolescents, especially when the adolescent tries to compare his or her peers by enduring the same pain (Suyemoto, 1998) or on the internet, where this behavior is being even celebrated in certain groups (Mitchell & Ybarra, 2007).
Despite the prevalence of this phenomenon among teens, only a very small percentage of adolescents who do self-harm use the medical or psychological help (Ystgaard et al., 2009; Hawton et al., 2002, Hrubá et al. 2012). Our study tries to reveal whether previous or current own experience of self-injurious individuals with professional psychological or psychiatric care is related to the occurrence, development or self-harm forms of behavior.
Research Methods
Based on the above concepts that highlight the diversity of aspects leading to self-harming behavior, the question arises whether there are significant differences between those adolescents who do the self-harm and have never been in the professional care of a psychiatrist or psychologist and those who were given a help from any reason in their personal history. In our study, we focused on exploring these possible connections and on the occurrence, development and duration of self- harm behavior. Furthermore, we wondered whether there can be found any characteristic types of self-harm behavior among the adolescents in professional psychological or psychiatric care.
Purpose of The Study
Self-harm among adolescents is a very serious phenomenon. Currently, there are many studies that deal with this issue. However, associated with previous or current psychological or psychiatric care, they are not completely mapped. We consider it essential to try to reveal whether a connection exists and expand our knowledge about self-harm. Furthermore, the results can be used to specify support for adolescents who self-harm.
Research Methods
The study was designed as a single cross-sectional survey with a sample of 1 110 adolescents aged 12-15 years (after alignment by age and sex). In our sample (n = 1 110 adolescents aged 12-15 years), 84 people stated that they were previously in contact with expert psychiatric or psychological care. There were 1 026 adolescents out of this care and 124 respondents stated an experience with self-harm. Respondents were assigned translated questionnaire SHI - Self-Harm Inventory (Sansone, Sansone, & Wiederman, 1995) that contains 22 items that relate to different types of self-harm. Some items, due to use by adolescents, excluded. A question was added to this questionnaire whether the teen currently or in his or her history took a psychological or psychiatric care.
Findings
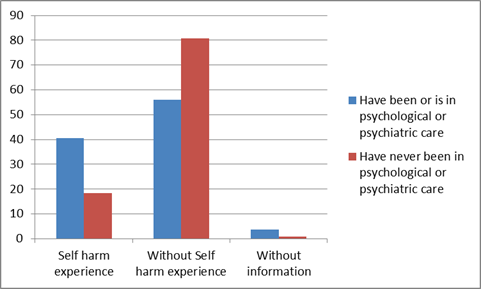
The first hypothesis we have asked is whether the adolescents, who have or have had contact with an expert in the field of psychology and psychiatry, have a higher incidence of self-harm behavior. Results in our sample point to the increased incidence of this type of behavior. Those teens, who have never been in care and are not, report their own experience with self-harm behavior in less than 20% while those, who were in care, report their own experience in 40% (Figure 1). Given behavior seems to act as a way how to reduce tension, relieve tension and is used as an inappropriate coping mechanism.
Next, we examined trends in the development of self-harm behavior. We found that the onset of self-harm, end of self-harm behavior is not significantly (at level p<0,05) different among adolescents, who have ever been or are in the care of psychologists and psychiatrists, from those who are not (table 1).
The most interesting indicator is the difference between the frequencies of use of self-harm behavior (table 2). According to the 14 selected modes of self-harm in the questionnaire SHI, we found, in each group, three groups according to the frequency of damage (0, 1-4, 5+). The results are noticeable different in the category of multiple occurrences (5 or more). In this category, the vastly greater number of adolescents (39.3%) who are, or have been in the past, in the professional care of a psychiatrist or psychologist compared to those who did not and will not use the service (23.4%). That means that the adolescents in this group not only have more frequent own experience with self-harm, but are also significantly represented in the group of adolescents who apply this behavior repeatedly and long-term. This shows the cyclical nature of self-harm behavior, which Chapman et al. (2006) outlines in his model Experiential avoidance model (EAM) of deliberate self-harm.
We can find a large number of self-harm behaviors. The most frequent are self-cutting (very often in the wrist and forearm), self-beating, self-stubbing or strikes to the head (Hrubá, Klimusová, & Burešová, 2012). SHI defines 14 ways of self-harm. All of them we processed by using contingency tables and chi-square. We will mention more those which have appeared significantly. These are: self-cutting, self-beating, striking to the head, worsening of health condition, drug abuse, serious injuries, attempted suicide and thought maltreatments.
Among adolescents, who have been or are in the professional care, there are 31% of people who sometimes cut themselves. This is a major difference compared to 16.9% of adolescents, who are not in professional care (relationship expressed by Cramer's V = 0.1 at level p <0.01, table 3).
In the category of hitting, the difference is smaller, but still substantial. Teens, who are or were in the care of a specialist, beat themselves at 39.3%. Those who have not used the care are 25.1% (table 4). For the specific category of "strikes to the head", the usage of this used among adolescents, who are or have been in the professional care, is 28.6%. For teens who are not in professional care, the result is 12.3% (table 5).
Interesting results are also opening up to us in not very traditional categories of self-harm, such as deterioration of health and drug abuse. Teens, who have been or are in the professional care of a psychologist or psychiatrist, worsen their health condition in 15.5% which is a striking difference from adolescents who never used the care - here is the presence of only 6.5% (table 6). Drugs abusing among adolescents, who were or are in the professional care of the psychological and psychiatric care represents 7.1% and the rest of 1,9% represents adolescents without care (table 7).
Conclusions
It is evident that the difference between adolescents who self-harm and find themselves in the care of experts in psychiatry and psychology, and those that do not use the service exists. Our research shows that teens, who reported that they were or are in contact with psychological and psychiatric experts considerably more likely tend to self-harm, and that this behavior is applied more and in more serious forms such as self-cutting, self-beating, striking to the head and last but not least, a very specific categories of self-harm such as worsening of health and drug abuse. On the contrary, no difference was found in the development of self-harm behavior. This finding is significant for both the laical and professional public and can help to find practical applications for working with risky adolescents in this age group.
Among the limitations of the study is has to be noted that the research sample of respondents cannot be considered representative. The selection of respondents was occasional (data was obtained through addressed school facilities). Furthermore, the limit of this research is also a school environment where questionnaires were scanned - in the classrooms. The results may thus be distorted by the lack of privacy, social adaptability or the possible time limit for completion.
This work unveiled the new context of self-harm. The relationship between previous or current professional care and self-harm behavior deserves the attention in further research. It offers, for example, to track causality of the relationship or connection of a specific focus of psychological or psychiatric care, its duration and self-harming. It would also be appropriate to explore this issue qualitatively, because there is another question of consulting methods and their impact on the development of self-harm.
Acknowledgements
The author(s) declare that there is no conflict of interest.
References
Bartošová, K. (2014). Psychické markery sebepoškozování v souvislosti s formou rodiny a rodičovským výchovným stylem (Dizertační práce). Brno: Masarykova Universita.
Bertolote, J. M. & Fleischmann, A. (2002). Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry, 1, 181–85.
Carli, V., Jovanovic, N., Podlešek, A., Rihmer, Z., Maggi, S., Marusic, D., Cesaro, C., Marusic, A., & Sarchiapone, M. (2010). The role of impulsivity in selfmutilators, suicide ideators and suicide attempters — A study of 1265 male incarcerated individuals. Journal of Affective Disorders, 123, 116- 122. DOI:
Chapman, A. L., Gratz, K. L., & Brown, M. Z. (2006). Solving the puzzle of deliberace sefl-harm: The experiential avoidance model. Behaviour Research and Therapy, 44(3), 371-394. DOI:
Evren, C., & Evren, B. (2005). Self-mutilation in substance-dependent patients and relationship with childhood abuse and neglect, alexithymia and temperament and character dimensions of personality. Drug and Alcohol Dependence, 80, 15- 22. DOI:
Favazza, A. R. (1987). Bodies under siege. Self- mutilation in culture and psychiatry. London: John Hopkins University Press.
Favazza, A. (1998). The coming of age of self-mutilation. The Journal of Nervous and Mental Disease, 186(5), 259–268. DOI:
Hawton, K., Rodham, K., Evans, E., & Weatherall, R. (2002). Deliberate self harm in adolescents: self report survey in schools in England. British Medical Journal, 325, 1207- 1211. DOI:
Himber, J. (1994). Blood rituals: Self-cutting in female psychiatric inpatients. Psychotherapy, 31, 620–631. DOI:
Hrubá, V., Klimusová, H., & Burešová, I. (2012). Výskyt, formy a vybrané souvislosti sebepoškozování u dětí staršího školního věku. In Halama, Peter; Hanák, Róbert; Masaryk, Radomír. Sociálne procesy a osobnosť 2012. Bratislava: Ústav experimentálnej psychológie SAV, 118-122.
Izutsu, T., Shimotsu, S., Matsumoto, T., Okada, T., KIKUCHI, A., & KOJIMOTO, M., et al. (2006). Deliberate Self-harm and Childhood Hyperactivity in Junior High School Students. European Child & Adolescent Psychiatry, 15(3), 172-176. DOI:
Janis, I. B., & Nock, M. K. (2008). Behavioral Forecasts Do Not Improve the Prediction of Future Behavior: A Prospective Study of Self-Injury. Journal of Clinical Psychology, 64(10), 1164-1174. DOI:
Kriegelová, M. (2008). Záměrné sebepoškozování v dětství a adolescenci. Praha: Grada Publishing, a.s.
Kvernmo, S., & Rosenvinge, J. H. (2009). Self-mutilation and suicidal behaviour in Sami and Norwegian adolescents: prevalence and correlates. International Journal of Circumpolar Health, 68(3), 235-248. DOI:
Lieberman, R. (2004). Understanding and Responding to Students Who Self-Mutilate. Principal Leadership, 4(7), 10-13.
Mitchell, K. J., & Ybarra, M. L. (2007). Online behavior of youth who engage in self-harm provides clues for preventive intervention. Preventive Medicine, 45, 392- 396. DOI:
Messer, J. M., & Rremouw, W. J. (2008). A critical review of explanatory models for selfmutilating behaviors in adolescents. Clinical Psychology Review, 28, 162- 178. DOI:
Platznerová, A. (2009). Sebepoškozování: Aktuální přehled diagnostiky, prevence a léčby. Praha: Galén
Sansone, R. A., Sansone, L. A., & Wiederman, M. W. (1995). The prevalence of trauma and its relationship to borderline personality symptoms and self-destructive behaviors in a primary care setting. Archives of Family Medicine, 4, 439–442. DOI:
Skegg, K. (2005). Self- harm. Lancet, 366, 1471- 1483. DOI:
Suyemoto, K. L. (1998). The function of self- mutilation. Clinical Psychology Review, 18(5), 531- 554. Ystgaard, M., Arensman, E., Hawton, K., Madge, N., Heeringen, K. V., Hewitt, A., Wilde, E. J. D., De. DOI:
Leo, D., & Fekete, S. (2009). Deliberate self-harm in adolescents: Comparison between those who receive help following self-harm and those who do not. Journal of Adolescence, 32, 875- 891. DOI:
Whitlock, J. (2010). What is self-injury? [Fact sheet] Cornell Research Program on Self-Injurious Behavior in Adolescents and Young Adults. Retrieved October 9, 2012, from http://crpsib.com/factsheet_aboutsi.asp
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.